Management of Infections with Multi-drug Resistance Bacteria การร กษาการต ดเช อแบคท เร ยด อยา
|
|
|
- Horace Armstrong
- 6 years ago
- Views:
Transcription

1 Management of Infections with Multi-drug Resistance Bacteria การร กษาการต ดเช อแบคท เร ยด อยา รองศาสตราจารย แพทย หญ งศศ โสภ ณ เก ยรต บ รณก ล คณะแพทยศาสตร โรงพยาบาลรามาธ บด Sasisopin Kiertiburanakul, MD, MHS Associate Professor Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University 2 nd IC on Stage, Nakornthon Hospital (November 29, 2012)
2 Outline Introduction Bacterial resistance Current guidelines Antibiotic options
3 Most Popular in Your Hospital A. A. baumannii B. P. aeruginosa C. ESBLs-producing Gram-negative bacteria

4 Superbug on IDSA hit list Enterococcus S. aureus K. pneumoniae A. baumannii P. aeruginosa E. cloacae Boucher HW et al. Clin Infect Dis 2009;48:1-12.
5 Bad Gram-negative Bugs Fermentative gram negative bacteria Enterobacteriaceae Klebsiella, Escherichia, Enterobacter, Salmonella, Shigella Proteus, Citrobacter, Serratia, Morganella, Yersinia, Edwardsiella, Providencia Non-fermentative gram negative bacteria P. aeruginosa Acinetobacter spp. Stenotrophomonas maltophilia
6 Bad Gram-Positive Bugs Methicillin-resistant Staphylococcus aureus (MRSA) 1 Methicillin-resistant coagulase-negative Staph (CoNS) 1 Vancomycin-resistant enterococci (VRE) 1 Penicillin-resistant Streptococcus pneumoniae 1 Clostridium difficile 2 1. Infectious Diseases Society of America. 2004: available on-line: 2. Peterson LP. Clin Infect Dis 2009;49:992-3.
7 Definitions Multidrug resistance (MDR) Non-susceptible to >1 agent in >3 antimicrobial categories* Extensive drug resistance (XDR) Non-susceptibility >1 agent in all but <2 antimicrobial categories* Pandrug resistance (PDR) Non-susceptibility to all agents in all antimicrobial categories* for each bacteria *List of antimicrobial agents used to treat the infections caused by this bacteria Falagas ME et al. Clin Infect Dis 2008;46: Magiorakos AP et al. Clin Microbiol Infect doi: /j x

8 Magiorakos AP et al. Clin Microbiol Infect 2012;18: X= non-susceptible
9 Susceptibility of E. coli Percentage (%) AMOX/CLAV CFR CRO CAZ NFX AMK GEN TMP/SMX National Antimicrobial Resistance Surveillance Center, Thailand
10 Susceptibility of A. baumannii 100 Percentage (%) CPZ/SUL IMP National Antimicrobial Resistance Surveillance Center, Thailand
11 Ramathibodi Antibiogram: June 2012 Organisms Ceftri Ceftaz Pip/tazo Imip Dori Cipro Amik A. baumannii E. cloacae E. coli K. pneumoniae P. aeruginosa S. maltophilia* *levofloxacin 85%, co-trimoxazole 82%
12 Nakornthon Antibiogram 2011 Organisms Ceftri Ceftaz Cef/sub Imip Cipro Amik A. baumannii Enterobacter spp E. coli K. pneumoniae P. aeruginosa S. maltophilia* *levofloxacin 92%, co-trimoxazole 71%


13 Mechanisms of Resistance of GNB Peleg AY, et al. N Engl J Med 2010;362:
14 Risk Factors for Resistance Health care associated infections Hospitalization for 2 days in preceding 90 days Residence in a nursing home or long-term care facility Home infusion therapy, including antimicrobial agents Long-term dialysis within 30 days Home wound care Family member with multidrugresistant pathogen Infection with drug-resistant bacteria Antimicrobial therapy in preceding 90 days Current hospitalization for 5 days High frequency of antibiotic resistance in the community or in the specific hospital unit Immunosuppression Guidelines for the management of adults with hospital-acquired, ventilator associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005;171:
15 Clinical Outcome of Mortality Resistant organism KPN-ESBL+ Non-resistant organism KPN-ESBL- P-value Bacteremia 1* 52% (n=48) 29% (n=99) AB (IMP-R) AB (IMP-S) Bacteremia % (n=40) 27.5% (n=40) <0.05 MDR-Pae No-MDR-Pae Bacteremia 3 21% (n=82) 12% (n=82) 0.08 EB (IMP-R) EB (IMP-S) Multiple sources 4 11% (n=33) 3% (n=33) KPN=K. pneumoniae; ESBL=extended-spectrum β-lactamase; AB=A. baumannii; IMP=imipenem; R=resistant; S=susceptible; Pae=P. aeruginosa; EB=Enterobacter spp. *95% CI, Tumbarello M et al. Antimicrob Agents Chemother 2006;50: Kwon KT et al. J Antimicrob Chemother 2007;59: Aloush V et al. Antimicrob Agents Chemother 2006;50: Marchaim D et al. Antimicrob Agents Chemother 2008;52:
16 Mortality Associated with Initial Inadequate Therapy in Critically Ill ICU Patients Alvarez-Lerma, 1996 Luna, 1997 Initial adequate therapy Initial inadequate therapy Rello, 1997 Kollef, 1998 Ibrahim, 2000** Harbarth, 2003 Valles, 2003** Mortality* 0% 20% 40% 60% 80% *Mortality refers to crude or infection-relate mortality- ** Patients had blood stream infections rather than pneumonia as in the other studies Intensive Care Med 1996;22: Chest 1997;111: Am J Respir Crit Care Med 1997;156: Chest 1996;113: Chest 2000;118: Am J Med 2003:115: Chest 2003;123:
17 Current Guidelines
18 Current Guidelines Hospital-acquired pneumonia Diabetes foot infection Intra-abdominal infection Complicated urinary tract infection
19 Hospital-, Ventilator-, and Healthcare-associated Pneumonia HAP: pneumonia that occurs 48 hours or more after admission, which was not incubating at the time of admission VAP: pneumonia that arises >48 72 hours after endotracheal intubation HCAP: hospitalized in acute care hospital >2 days within 90 days, resided in nursing home or longterm care facility, received recent IV antibiotic therapy, chemotherapy, or wound care within the past 30 days, or attended hospital or hemodialysis clinic ATS, IDSA. Am J Respir Crit Care Med 2005;171:
20 Hospital-, Ventilator-, and Healthcare-associated Pneumonia Aerobic gram-negative bacilli P. aeruginosa, E. coli, K. pneumoniae, and Acinetobacter spp. Gram-positive cocci S. aureus, MRSA Polymicrobial infection Multidrug-resistance pathogens Antimicrobial therapy in preceding 90 days Current hospitalization >5 days High frequency of resistance in community or specific hospital unit Presence of risk factors for HCAP Immunosuppressive disease and/or therapy ATS, IDSA. Am J Respir Crit Care Med 2005;171:
21 ATS/IDSA Guideline: Empiric Therapy HAP, VAP or HCAP suspected (all disease severity) Late onset (>5 days) or risk factors for MDR pathogens No Yes Limited spectrum antibiotic therapy Broad spectrum antibiotic therapy for MDR pathogens ATS, IDSA. Am J Respir Crit Care Med 2005;171:
22 Risk Factors for MDR Pathogens or Late Onset ATS, IDSA. Am J Respir Crit Care Med 2005;171:
23 Nosocomial Pneumonia Treatment Caused by MDR Pathogens Jean SS et al. Expert Opin Pharmacother 2011;12:


24 Solomkin JS et al. Clin Infect Dis 2010;50:
25 Complicated Intra-abdominal Infections Perforated intestines, intra-abdominal abscesses, appendicitis, diverticulitis, or cholecysitis with perforation and/or abscess with fecal contamination, or perforated gastric/duodenal ulcers, and complicated peritonitis Healthcare-associated infections generally require broader antibacterial coverage P. aeruginosa, Enterobacter spp. and MRSA Objectives for the treatment: to minimize time to clinical improvement, prevent recurrence, and eradicate causative microorganisms

26 Complicated Intra-abdominal Infections Solomkin JS et al. Clin Infect Dis 2010;50:

27 Recommendations for Empirical Therapy Solomkin JS et al. Clin Infect Dis 2010;50:

28 Urinary Tract Infections Hsueh PR et al. J Infect 2011;63:

29 Empirical Antimicrobial Therapy e: for multidrug-resistant Enterobacteriaceae and A. baumannii and vancomycin-resistant enterococci. f: for multidrug-resistant Enterobacteriaceae, P. aeruginosa, and A. baumannii. Hsueh PR et al. J Infect 2011;63:
30 Antibiotic Selection
31 Consensus Prescribing Principles Appropriate and effective prescribing guidelines TREAT OPTIMIZE MAXIMIZE RECOGNIZE UTILIZE INTEGRATE bacterial infection only diagnosis/severity assessment bacterial eradication (local) resistance prevalence pharmacodynamics - for effective agents and dosage local resistance, efficacy and cost-effectiveness Ball et al. J Antimicrob Chemother 2002;49:31 40.
32 Factors to Consider When Selecting Antibiotics Spectrum Prove clinical efficacy PK/PD Convenience/compliance Cost Adverse effects Antibiotic factors Disease specific factors Patients factors Previous ATB Age Concomitant diseases Pregnancy Drug allergy Possible pathogens Likelihood of resistance Severity of infection
33 Comparison of Antimicrobial Spectra Organism 3rd/4th Cephalosporins BL/BI Carbapenems Ceftazidime Cefepime Pip/tazo Doripenem Imipenem Meropenem Ertapenem Gram-Positive: S. pneumoniae MSSA +/ E. faecalis /- + +/- 0 E. faecium +/- 0 +/- 0 0 Gram-Negative: E. coli Klebsiella spp E.coli /Kleb spp. ESBL / Enterobacter spp Proteus spp Acinetobacter spp. +/- +/- +/- +/- +/- +/- 0 P. aeruginosa Anaerobes: B. fragilis Clostridium (not difficile) Peptostreptococcus spp The Sanford Guide to Antimicrobial Therapy = usually effective clinically or >60% susceptible; +/- = clinical trail lacking or 30-60% susceptible 0= not effective clinically or <30% susceptible; blank = data not available

34 Local Antibiogram: iphone Application
35 What to Treat? ESBLs Imipenem Meropenem Doripenem Ertapenem Peleg AY et al. N Engl J Med 2010;362:
36 Management Options: ESBLs Antimicrobial agent Pros Cons Carbapenems Fluoroquinolones Drug of choice for severe infections Option for non-serious UTIs, if sensitive Ertapenem-less susceptible; overuse? Empirical use-not recommended Aminoglycosides Effective if sensitive Avoided monotherapy Fosfomycin Tigecycline β-lactamase inhibitor combinations Option for UTIs, oral form (cystitis) Excellent in vitro activity against ESBL producers May be active against ESBL producers, UTIs Conjunction with other antibiotics for other infections, less clinical data FDA warned against its use for serious HAP/VAP, less clinical data Should not used for serious infections Polymixins Excellent efficacy Nephrotoxicity Modified from Dhillon RH et al. Crit Care Res Pract 2012;2012:
37 What to Treat? ESBLs Imipenem Meropenem Doripenem Ertapenem Carbapenemase-producing Enterobacteriaceae Colistin Tigecycline Combination with others Carbapenem-resistant P. aeruginosa Carbapenem-resistant A. baumannii Colistin Extended infusion of carbapenem Combination with others Colistin Tigecycline Sulbactam combination Extended infusion of carbapenem Combination with others Peleg AY et al. N Engl J Med 2010;362:
38 Other Options
39 Combat to Antibiotic-resistant Pathogens New drugs Increased dose Increased frequency Prolonged or continuous infusion Combination anitibiotics
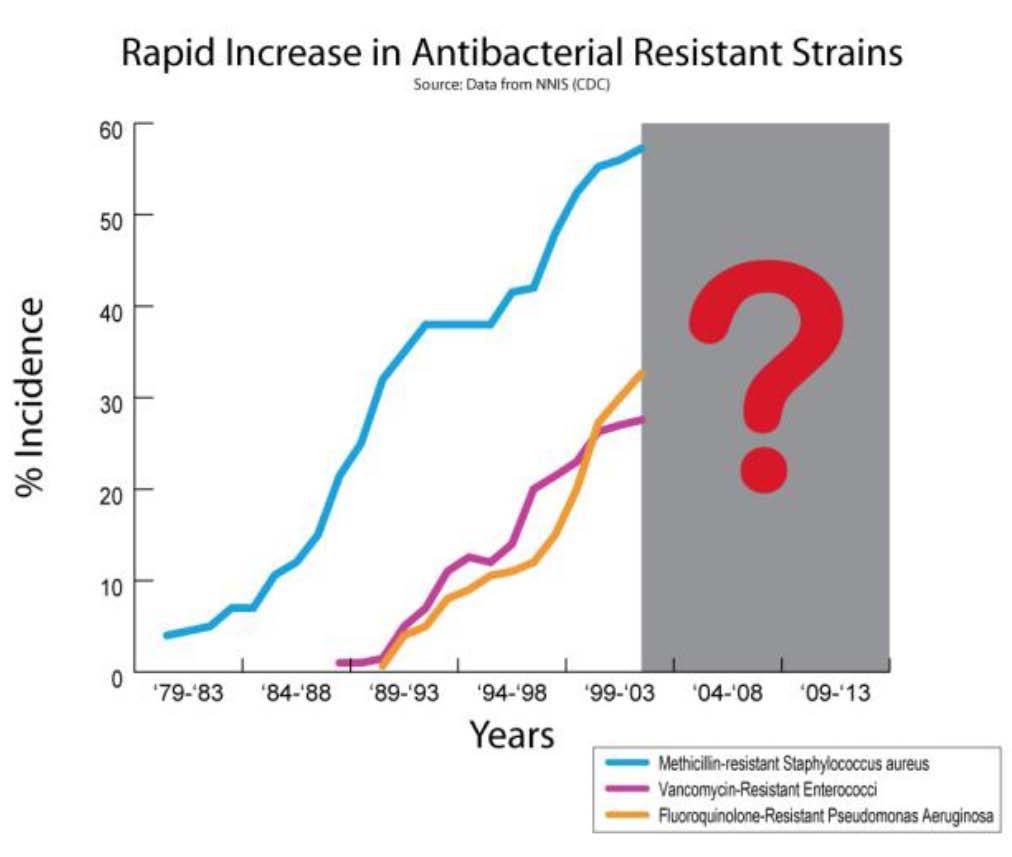
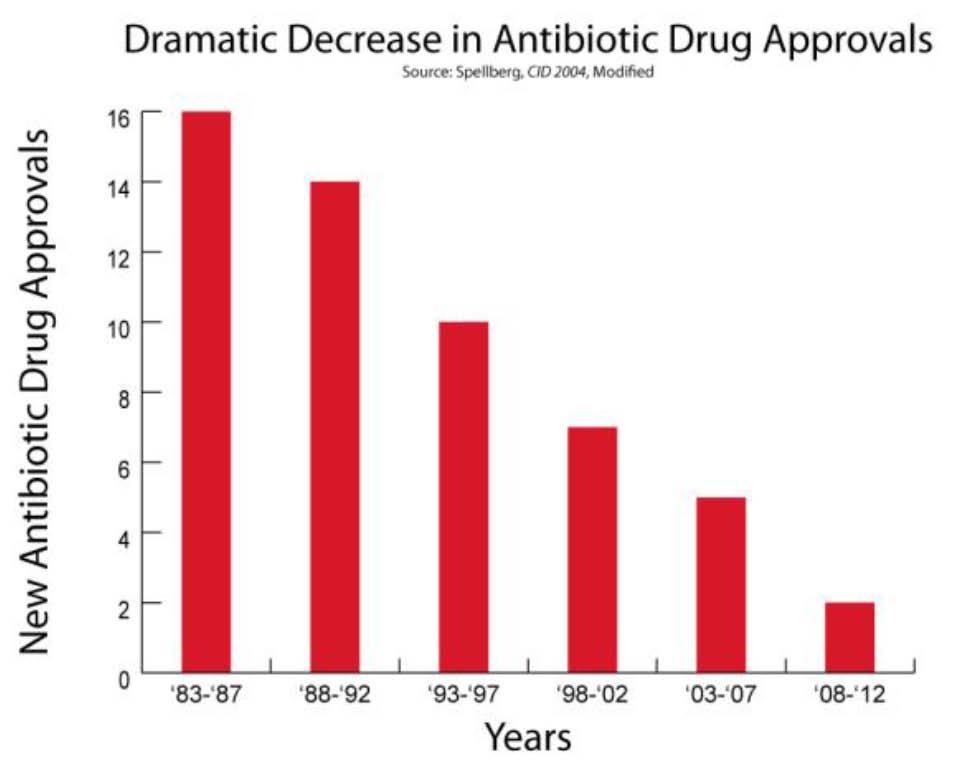
40 Problems!!! Bad_Bugs_No_Drugs/Press_Releases/Antibiotic%20Resistance%20Fact%20Sheet.pdf
41 Dosage of Antibiotics: HAP, VAP, HCAP Doripenem 500 mg every 8 h Dosages are based on normal renal and hepatic function Trough levels for gentamicin and tobramycin should be less than 1 g/ml, and for amikacin they should be less than 4 5 g/ml Trough levels for vancomycin should be g/ml ATS, IDSA. Am J Respir Crit Care Med 2005;171:
42 β-lactams Antibiotics T >MIC (% of dosing interval) C max (Peak) Serum level Serum Concentration Time above MIC MIC = 4 C min (Trough) MIC = 2 Time 6 hours
43 Time-dependent Killing %T>MIC <50% %T>MIC >50% MIC 90 MIC 90 More frequent infusion %T>MIC = 100% %T>MIC >50% 32 MIC MIC 90 Continuous infusion Prolonged infusion Modified from and Courtesy of Koomanachai P.
44 Prolonged or Continuous Infusion Extending infusion time, antibiotic levels will be sustained above MIC of targeted organisms 1,2 May potentially result in improved drug efficacy Improve clinical outcomes for meropenem (cure rate 90.5% vs. 59.6%; P <0.001) 3 Prolonged infusion consistently achieved higher pharmacodynamic endpoints 4 Improved clinical outcomes in subgroup of P. aeruginosa infection and APACHE >17 Prospective randomized trial: doripenem 4-hour infusion vs imipenem 30/60-minutes infusion 5 Reduction in development of resistant P. aeruginosa 1. Lodise TP et al. Pharmacotherapy 2006;26: Kim A et al. Pharmacotherapy 2007;27: Lorente L et al. Ann Pharmacother 2006;40: Mah GT et al. Ann Pharmacother 2012;46: Chastre J et al. Crit Care Med 2008;36:
45 Prolonged Infusion for MDR Organisms Piperacillin/tazobactam g q 6-8 hr, drip 3-4 hr 1,2 Continuous infusion Cefepime: 2 g q 8 hr, drip 3 hr 3 Ceftazidime: 2 g q 8 hr, drip 3 hr 4 Meropenem: 2 g q 8 hr, drip 3 hr 4 Imipenem: 500 mg or 1 g q 8 hr, drip 2-3 hr 5 Doripenem: 500 mg q 8 hr, drip 4 hr 1.Kim A et al. Pharmacotherapy 2007;27: Lodise TP Jr et al. Clin Infect Dis 2007;44: Crandon JL et al. Ann Pharmacother 2009;43: Kiim A et al. Clin Ther 2009;31: Jaruratanasirikul S et al. J Antimicrob Chemother 2009;63:560-3.
46 Why Empiric Combination Therapy? A. Synergistic B. More coverage C. Prevent/minimize drug resistance
47 Combination Therapy: Why? Severe infection or critically-ill patient Optimize coverage Exact pathogen is unknown Immunoduratory effect? Prevent emergence of resistance? Synergistic effect? Overuse resistance

48 Optimize Spectrum Coverage Micek ST et al. Antimicrob Agents Chemother 2010;54:
49 Combination Therapy and MDR A. baumannii Yoon J et al. Antimicrob Agents Chemother 2004;48:
50 Combination vs. Monotherapy for Empiric Therapy PRO Synergistic effect in vitro Good outcome in severely ill Septic shock, neutropenia, infection with MDR organisms Higher rate of microbiological cure CON Higher rates of resistance isolates Higher rates of side effects Lack of the power to showed consistent of good outcome No top-level evidence to support or reject* *Kollef MH et al. Clin Infect Dis 2011;53:S33 S55.
51 Combination Therapy: Suggestion For patients who are critically ill and in institutions with high rates of antibiotic resistance Empiric combination therapy is justified If use, not delay! * Early de-escalation to targeted monotherapy when susceptibilities are known With active β-lactam *Kumar A et al. Crit Care Med 2010;38:

52 A Patient with VAP
53 VAP with MDR Pathogens
54 Your Choice A. Combination B. Extended infusion C. Both
55 Vancomycin and S. aureus MSSA Inferior to at least some β-lactams for the treatment of bacteremia and endocarditis MRSA MIC creep Poor therapeutic response Limitations of the clinical lab in detecting reduced susceptibility and resistance Poor penetration into tissue Increasing dose may not safely overcome its poor activity and limited tissue penetration Inferior to some comparators in randomized control trials Combination with a second anti-staphylococcal antibiotic does not improve its therapeutic efficacy Deresinski S. Clin Infect Dis 2007;44:154-8.
56 Monitoring of Vancomycin IV vancomycin mg/kg/dose (actual body weight) every 8-12 h, not to exceed 2 g per dose Trough serum vancomycin concentrations Just before the 4 th or 5 th dose Should always be maintained >10 µg/ml to avoid development of resistance µg/ml are recommended to improve penetration In seriously ill patients, a loading dose of mg/kg Recommended Patients receiving aggressive dosing High risk of nephrotoxicity or unstable renal function Receiving prolonged courses of therapy Raybak M et al. Am J Health-Syst Pharm 2009;66:82-98.
57 Summary 1 Resistance should be a concern issue in clinical practice Infection with bacterial resistance is a leading cause of inadequate treatment and mortality Prompt empiric antimicrobial agents
58 Summary 2 Appropriate and adequate uses of antimicrobial agents Choosing antimicrobial agent depends on clinical indications, patients condition, and drugs profiles Streamline therapy Prolonged infusion and combination when appropriate



59 The WHO SAVE LIVES: Clean Your Hands
Appropriate antimicrobial therapy in HAP: What does this mean?
 Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
Appropriate antimicrobial therapy in HAP: What does this mean? Jaehee Lee, M.D. Kyungpook National University Hospital, Korea KNUH since 1907 Presentation outline Empiric antimicrobial choice: right spectrum,
4/3/2017 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA DISCLOSURE LEARNING OBJECTIVES
 CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
CLINICAL PEARLS: UPDATES IN THE MANAGEMENT OF NOSOCOMIAL PNEUMONIA BILLIE BARTEL, PHARMD, BCCCP APRIL 7 TH, 2017 DISCLOSURE I have had no financial relationship over the past 12 months with any commercial
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia. Po-Ren Hsueh. National Taiwan University Hospital
 Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Update on Resistance and Epidemiology of Nosocomial Respiratory Pathogens in Asia Po-Ren Hsueh National Taiwan University Hospital Ventilator-associated Pneumonia Microbiological Report Sputum from a
Mono- versus Bitherapy for Management of HAP/VAP in the ICU
 Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Mono- versus Bitherapy for Management of HAP/VAP in the ICU Jean Chastre, www.reamedpitie.com Conflicts of interest: Consulting or Lecture fees: Nektar-Bayer, Pfizer, Brahms, Sanofi- Aventis, Janssen-Cilag,
Management of Hospital-acquired Pneumonia
 Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
Management of Hospital-acquired Pneumonia Adel Alothman, MB, FRCPC, FACP Asst. Professor, COM, KSAU-HS Head, Infectious Diseases, Department of Medicine King Abdulaziz Medical City Riyadh Saudi Arabia
2012 ANTIBIOGRAM. Central Zone Former DTHR Sites. Department of Pathology and Laboratory Medicine
 2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
2012 ANTIBIOGRAM Central Zone Former DTHR Sites Department of Pathology and Laboratory Medicine Medically Relevant Pathogens Based on Gram Morphology Gram-negative Bacilli Lactose Fermenters Non-lactose
Outline. Antimicrobial resistance. Antimicrobial resistance in gram negative bacilli. % susceptibility 7/11/2010
 Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Multi-Drug Resistant Organisms Is Combination Therapy the Way to Go? Sutthiporn Pattharachayakul, PharmD Prince of Songkhla University, Thailand Outline Prevalence of anti-microbial resistance in Acinetobacter
Learning Points. Raymond Blum, M.D. Antimicrobial resistance among gram-negative pathogens is increasing
 Raymond Blum, M.D. Learning Points Antimicrobial resistance among gram-negative pathogens is increasing Infection with antimicrobial-resistant pathogens is associated with increased mortality, length of
Raymond Blum, M.D. Learning Points Antimicrobial resistance among gram-negative pathogens is increasing Infection with antimicrobial-resistant pathogens is associated with increased mortality, length of
Intrinsic, implied and default resistance
 Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
Appendix A Intrinsic, implied and default resistance Magiorakos et al. [1] and CLSI [2] are our primary sources of information on intrinsic resistance. Sanford et al. [3] and Gilbert et al. [4] have been
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases
 The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
The International Collaborative Conference in Clinical Microbiology & Infectious Diseases PLUS: Antimicrobial stewardship in hospitals: Improving outcomes through better education and implementation of
Antibiotic Updates: Part II
 Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part II Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Mercy Medical Center Des Moines, Iowa Department of Pathology. Microbiology Department Antibiotic Susceptibility January December 2016
 Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Mercy Medical Center Des Moines, Iowa Department of Pathology Microbiology Department Antibiotic Susceptibility January December 2016 These statistics are intended solely as a GUIDE to choosing appropriate
Antibiotic Abyss. Discussion Points. MRSA Treatment Guidelines
 Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Antibiotic Abyss Fredrick M. Abrahamian, D.O., FACEP, FIDSA Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California
Preserving bacterial susceptibility Implementing Antimicrobial Stewardship Programs Debra A. Goff, Pharm.D., FCCP
 Preserving bacterial susceptibility Implementing Antimicrobial Stewardship Programs Debra A. Goff, Pharm.D., FCCP Clinical Associate Professor Infectious Diseases Specialist The Ohio State University Medical
Preserving bacterial susceptibility Implementing Antimicrobial Stewardship Programs Debra A. Goff, Pharm.D., FCCP Clinical Associate Professor Infectious Diseases Specialist The Ohio State University Medical
SHC Clinical Pathway: HAP/VAP Flowchart
 SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
SHC Clinical Pathway: Hospital-Acquired and Ventilator-Associated Pneumonia SHC Clinical Pathway: HAP/VAP Flowchart v.08-29-2017 Diagnosis Hospitalization (HAP) Pneumonia develops 48 hours following: Endotracheal
Concise Antibiogram Toolkit Background
 Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Background This toolkit is designed to guide nursing homes in creating their own antibiograms, an important tool for guiding empiric antimicrobial therapy. Information about antibiograms and instructions
Fighting MDR Pathogens in the ICU
 Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Fighting MDR Pathogens in the ICU Dr. Murat Akova Hacettepe University School of Medicine, Department of Infectious Diseases, Ankara, Turkey 1 50.000 deaths each year in US and Europe due to antimicrobial
Safe Patient Care Keeping our Residents Safe Use Standard Precautions for ALL Residents at ALL times
 Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Safe Patient Care Keeping our Residents Safe 2016 Use Standard Precautions for ALL Residents at ALL times #safepatientcare Do bugs need drugs? Dr Deirdre O Brien Consultant Microbiologist Mercy University
Witchcraft for Gram negatives
 Witchcraft for Gram negatives Dr Subramanian S MD DNB MNAMS AB (Medicine, Infect Dis) Infectious Diseases Consultant Global Health City, Chennai www.asksubra.com Drug resistance follows the drug like a
Witchcraft for Gram negatives Dr Subramanian S MD DNB MNAMS AB (Medicine, Infect Dis) Infectious Diseases Consultant Global Health City, Chennai www.asksubra.com Drug resistance follows the drug like a
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE
 PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
PRACTIC GUIDELINES for APPROPRIATE ANTIBIOTICS USE Global Alliance for Infection in Surgery World Society of Emergency Surgery (WSES) and not only!! Aims - 1 Rationalize the risk of antibiotics overuse
Antimicrobial Susceptibility Testing: Advanced Course
 Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Testing: Advanced Course Cascade Reporting Cascade Reporting I. Selecting Antimicrobial Agents for Testing and Reporting Selection of the most appropriate antimicrobials to
Antimicrobial Susceptibility Patterns
 Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
Antimicrobial Susceptibility Patterns KNH SURGERY Department Masika M.M. Department of Medical Microbiology, UoN Medicines & Therapeutics Committee, KNH Outline Methodology Overall KNH data Surgery department
UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients
 Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Background/methods: UCSF guideline for management of suspected hospital-acquired or ventilatoracquired pneumonia in adult patients This guideline establishes evidence-based consensus standards for management
Other Beta - lactam Antibiotics
 Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Other Beta - lactam Antibiotics Assistant Professor Dr. Naza M. Ali Lec 5 8 Nov 2017 Lecture outlines Other beta lactam antibiotics Other inhibitors of cell wall synthesis Other beta-lactam Antibiotics
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Kaitlin McGinn, PharmD Assistant Clinical Professor, Critical Care Auburn University, Harrison School of Pharmacy November
Updates on the Management of Hospital Acquired Infections and Resistant Organisms
 Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
Updates on the Management of Hospital Acquired Infections and Resistant Organisms Conflict of Interest I, Kaitlin McGinn, have no actual or potential conflict of interest in relation to this program. Kaitlin
GENERAL NOTES: 2016 site of infection type of organism location of the patient
 GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GENERAL NOTES: This is a summary of the antibiotic sensitivity profile of clinical isolates recovered at AIIMS Bhopal Hospital during the year 2016. However, for organisms in which < 30 isolates were recovered
GORILLACILLINS IN THE ICU:
 Conflicts of Interest None to declare GORILLACILLINS IN THE ICU: From SPACE and Beyond... Tim T.Y. Lau, PharmD, FCSHP Clinical Pharmacy Specialist in Infectious Diseases Pharmaceutical Sciences, Vancouver
Conflicts of Interest None to declare GORILLACILLINS IN THE ICU: From SPACE and Beyond... Tim T.Y. Lau, PharmD, FCSHP Clinical Pharmacy Specialist in Infectious Diseases Pharmaceutical Sciences, Vancouver
Management of hospital-acquired acquired pneumonia in the Asian Pacific region
 Management of hospital-acquired acquired pneumonia in the Asian Pacific region Jae-Hoon Song, MD, PhD Samsung Medical Center Asian Network for Surveillance of Resistant Pathogens (ANSORP) Asian-Pacific
Management of hospital-acquired acquired pneumonia in the Asian Pacific region Jae-Hoon Song, MD, PhD Samsung Medical Center Asian Network for Surveillance of Resistant Pathogens (ANSORP) Asian-Pacific
2017 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2017 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Sustaining an Antimicrobial Stewardship
 Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Sustaining an Antimicrobial Stewardship Much needless expense, untoward effect, harm and disappointment can be prevented by better judgment in the use of antimicrobials Whitney A. Jones, PharmD Antimicrobial
Antimicrobial Cycling. Donald E Low University of Toronto
 Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Antimicrobial Cycling Donald E Low University of Toronto Bad Bugs, No Drugs 1 The Antimicrobial Availability Task Force of the IDSA 1 identified as particularly problematic pathogens A. baumannii and
Surgical infection ผ.ศ. น.พ. กำธร มำลำธรรม หน วยโรคต ดเช อ ภำคว ชำอำย รศำสตร คณะแพทยศำสตร โรงพยำบำลรำมำธ บด
 Surgical infection ผ.ศ. น.พ. กำธร มำลำธรรม หน วยโรคต ดเช อ ภำคว ชำอำย รศำสตร คณะแพทยศำสตร โรงพยำบำลรำมำธ บด 1 Scope Surgical prophylaxis: Pharmacologic approach to prevent SSI Antimicrobial therapy for
Surgical infection ผ.ศ. น.พ. กำธร มำลำธรรม หน วยโรคต ดเช อ ภำคว ชำอำย รศำสตร คณะแพทยศำสตร โรงพยำบำลรำมำธ บด 1 Scope Surgical prophylaxis: Pharmacologic approach to prevent SSI Antimicrobial therapy for
Antimicrobial Pharmacodynamics
 Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
Antimicrobial Pharmacodynamics November 28, 2007 George P. Allen, Pharm.D. Assistant Professor, Pharmacy Practice OSU College of Pharmacy at OHSU Objectives Become familiar with PD parameters what they
2015 Antibiogram. Red Deer Regional Hospital. Central Zone. Alberta Health Services
 2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
2015 Antibiogram Red Deer Regional Hospital Central Zone Alberta Health Services Introduction. This antibiogram is a cumulative report of the antimicrobial susceptibility rates of common microbial pathogens
Antibiotic Stewardship Program (ASP) CHRISTUS SETX
 CHRISTUS SETX") Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Antibiotic Stewardship Program (ASP) CHRISTUS SETX Program Goals I. Judicious use of antibiotics Decrease use of broad spectrum antibiotics and deescalate use based on clinical symptoms Therapeutic duplication:
Aberdeen Hospital. Antibiotic Susceptibility Patterns For Commonly Isolated Organisms For 2015
 Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
Aberdeen Hospital Antibiotic Susceptibility Patterns For Commonly Isolated s For 2015 Services Laboratory Microbiology Department Aberdeen Hospital Nova Scotia Health Authority 835 East River Road New
What s next in the antibiotic pipeline?
 What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
What s next in the antibiotic pipeline? Jennifer Tieu, Pharm.D., BCPS Clinical Pearls OSHP Spring Meeting Mercy Hospital April 13, 2018 Objective 2 Describe the drug class and mechanism of action of antibiotics
Antimicrobial stewardship: Quick, don t just do something! Stand there!
 Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Antimicrobial stewardship: Quick, don t just do something! Stand there! Stanley I. Martin, MD, FACP, FIDSA Director, Division of Infectious Diseases Director, Antimicrobial Stewardship Program Geisinger
Multi-drug resistant microorganisms
 Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
Multi-drug resistant microorganisms Arzu TOPELI Director of MICU Hacettepe University Faculty of Medicine, Ankara-Turkey Council Member of WFSICCM Deaths in the US declined by 220 per 100,000 with the
4 th and 5 th generation cephalosporins. Naderi HR Associate professor of Infectious Diseases
 4 th and 5 th generation cephalosporins Naderi HR Associate professor of Infectious Diseases Classification Forth generation: Cefclidine, cefepime (Maxipime),cefluprenam, cefoselis,cefozopran, cefpirome
4 th and 5 th generation cephalosporins Naderi HR Associate professor of Infectious Diseases Classification Forth generation: Cefclidine, cefepime (Maxipime),cefluprenam, cefoselis,cefozopran, cefpirome
2016 Antibiogram. Central Zone. Alberta Health Services. including. Red Deer Regional Hospital. St. Mary s Hospital, Camrose
 2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
2016 Antibiogram Central Zone Alberta Health Services including Red Deer Regional Hospital St. Mary s Hospital, Camrose Introduction This antibiogram is a cumulative report of the antimicrobial susceptibility
Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them?
 Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them? Roberta B. Carey, PhD Centers for Disease Control and Prevention Division of Healthcare Quality Promotion Why worry? MDROs Clinical
Multidrug-Resistant Organisms: How Do We Define them? How do We Stop Them? Roberta B. Carey, PhD Centers for Disease Control and Prevention Division of Healthcare Quality Promotion Why worry? MDROs Clinical
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections
 for the treatment of Acinetobacter baumannii infections") ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
ETX2514SUL (sulbactam/etx2514) for the treatment of Acinetobacter baumannii infections Robin Isaacs Chief Medical Officer, Entasis Therapeutics Dr. Isaacs is a full-time employee of Entasis Therapeutics.
Detecting / Reporting Resistance in Nonfastidious GNR Part #2. Janet A. Hindler, MCLS MT(ASCP)
") Detecting / Reporting Resistance in Nonfastidious GNR Part #2 Janet A. Hindler, MCLS MT(ASCP) Methods Described in CLSI M100-S21 for Testing non-enterobacteriaceae Organism Disk Diffusion MIC P. aeruginosa
Detecting / Reporting Resistance in Nonfastidious GNR Part #2 Janet A. Hindler, MCLS MT(ASCP) Methods Described in CLSI M100-S21 for Testing non-enterobacteriaceae Organism Disk Diffusion MIC P. aeruginosa
2016 Antibiotic Susceptibility Report
 Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
Fairview Northland Medical Center and Elk River, Milaca, Princeton and Zimmerman Clinics 2016 Antibiotic Susceptibility Report GRAM-NEGATIVE ORGANISMS 2016 Gram-Negative Non-Urine The number of isolates
2015 Antibiotic Susceptibility Report
 Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Citrobacter freundii Enterobacter aerogenes Enterobacter cloacae Escherichia coli Haemophilus influenzenza Klebsiella oxytoca Klebsiella pneumoniae Proteus mirabilis Pseudomonas aeruginosa Serratia marcescens
Summary of the latest data on antibiotic resistance in the European Union
 Summary of the latest data on antibiotic resistance in the European Union EARS-Net surveillance data November 2017 For most bacteria reported to the European Antimicrobial Resistance Surveillance Network
Summary of the latest data on antibiotic resistance in the European Union EARS-Net surveillance data November 2017 For most bacteria reported to the European Antimicrobial Resistance Surveillance Network
Treatment Guidelines and Outcomes of Hospital- Acquired and Ventilator-Associated Pneumonia
 SUPPLEMENT ARTICLE Treatment Guidelines and Outcomes of Hospital- Acquired and Ventilator-Associated Pneumonia Antoni Torres, Miquel Ferrer, and Joan Ramón Badia Pneumology Department, Clinic Institute
SUPPLEMENT ARTICLE Treatment Guidelines and Outcomes of Hospital- Acquired and Ventilator-Associated Pneumonia Antoni Torres, Miquel Ferrer, and Joan Ramón Badia Pneumology Department, Clinic Institute
BACTERIAL SUSCEPTIBILITY REPORT: 2016 (January 2016 December 2016)
") BACTERIAL SUSCEPTIBILITY REPORT: 2016 (January 2016 December 2016) VA Palo Alto Health Care System April 14, 2017 Trisha Nakasone, PharmD, Pharmacy Service Russell Ryono, PharmD, Public Health Surveillance
BACTERIAL SUSCEPTIBILITY REPORT: 2016 (January 2016 December 2016) VA Palo Alto Health Care System April 14, 2017 Trisha Nakasone, PharmD, Pharmacy Service Russell Ryono, PharmD, Public Health Surveillance
CF WELL Pharmacology: Microbiology & Antibiotics
 CF WELL Pharmacology: Microbiology & Antibiotics Bradley E. McCrory, PharmD, BCPS Clinical Pharmacy Specialist Pulmonary Medicine Cincinnati Children s Hospital Medical Center January 26, 2017 Disclosure
CF WELL Pharmacology: Microbiology & Antibiotics Bradley E. McCrory, PharmD, BCPS Clinical Pharmacy Specialist Pulmonary Medicine Cincinnati Children s Hospital Medical Center January 26, 2017 Disclosure
Dr. Shaiful Azam Sazzad. MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College
 Critical Care Medicine Dhaka Medical College") Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Dr. Shaiful Azam Sazzad MD Student (Thesis Part) Critical Care Medicine Dhaka Medical College INTRODUCTION ICU acquired infection account for substantial morbidity, mortality and expense. Infection and
Sepsis is the most common cause of death in
 ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
ADDRESSING ANTIMICROBIAL RESISTANCE IN THE INTENSIVE CARE UNIT * John P. Quinn, MD ABSTRACT Two of the more common strategies for optimizing antimicrobial therapy in the intensive care unit (ICU) are antibiotic
Antibiotic. Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting
 Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Antibiotic Antibiotic Classes, Spectrum of Activity & Antibiotic Reporting Any substance of natural, synthetic or semisynthetic origin which at low concentrations kills or inhibits the growth of bacteria
Available online at ISSN No:
 Available online at www.ijmrhs.com ISSN No: 2319-5886 International Journal of Medical Research & Health Sciences, 2017, 6(4): 36-42 Comparative Evaluation of In-Vitro Doripenem Susceptibility with Other
Available online at www.ijmrhs.com ISSN No: 2319-5886 International Journal of Medical Research & Health Sciences, 2017, 6(4): 36-42 Comparative Evaluation of In-Vitro Doripenem Susceptibility with Other
CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE)
") CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE) Bartsch SM et al. Potential economic burden of carbapenem-resistent Enterobacteriaceae (CRE) in the United States. Clin Microbiol Infect 2017;23(1):48e9-e16.
CARBAPENEM RESISTANT ENTEROBACTERIACEAE (KPC CRE) Bartsch SM et al. Potential economic burden of carbapenem-resistent Enterobacteriaceae (CRE) in the United States. Clin Microbiol Infect 2017;23(1):48e9-e16.
The β- Lactam Antibiotics. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
The β- Lactam Antibiotics Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 Penicillins. Cephalosporins. Carbapenems. Monobactams. The β- Lactam Antibiotics 2 3 How
Int.J.Curr.Microbiol.App.Sci (2017) 6(3):
 6(3):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 3 (2017) pp. 891-895 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.603.104
2010 ANTIBIOGRAM. University of Alberta Hospital and the Stollery Children s Hospital
 2010 ANTIBIOGRAM University of Alberta Hospital and the Stollery Children s Hospital Medical Microbiology Department of Laboratory Medicine and Pathology Table of Contents Page Introduction..... 2 Antibiogram
2010 ANTIBIOGRAM University of Alberta Hospital and the Stollery Children s Hospital Medical Microbiology Department of Laboratory Medicine and Pathology Table of Contents Page Introduction..... 2 Antibiogram
Bacterial infections complicating cirrhosis
 PHC www.aphc.info Bacterial infections complicating cirrhosis P. Angeli, Dept. of Medicine, Unit of Internal Medicine and Hepatology (), University of Padova (Italy) pangeli@unipd.it Agenda Epidemiology
PHC www.aphc.info Bacterial infections complicating cirrhosis P. Angeli, Dept. of Medicine, Unit of Internal Medicine and Hepatology (), University of Padova (Italy) pangeli@unipd.it Agenda Epidemiology
Surveillance for Antimicrobial Resistance and Preparation of an Enhanced Antibiogram at the Local Level. janet hindler
 Surveillance for Antimicrobial Resistance and Preparation of an Enhanced Antibiogram at the Local Level janet hindler At the conclusion of this talk, you will be able to Describe CLSI M39-A3 recommendations
Surveillance for Antimicrobial Resistance and Preparation of an Enhanced Antibiogram at the Local Level janet hindler At the conclusion of this talk, you will be able to Describe CLSI M39-A3 recommendations
Principles of Infectious Disease. Dr. Ezra Levy CSUHS PA Program
 Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
Principles of Infectious Disease Dr. Ezra Levy CSUHS PA Program I. Microbiology (1) morphology (e.g., cocci, bacilli) (2) growth characteristics (e.g., aerobic vs anaerobic) (3) other qualities (e.g.,
The role of new antibiotics in the treatment of severe infections: Safety and efficacy features
 The role of new antibiotics in the treatment of severe infections Safety and efficacy features Christian Eckmann Hannover, Germany The role of new antibiotics in the treatment of severe infections: Safety
The role of new antibiotics in the treatment of severe infections Safety and efficacy features Christian Eckmann Hannover, Germany The role of new antibiotics in the treatment of severe infections: Safety
5/4/2018. Multidrug Resistant Organisms (MDROs) Objectives. Outline. Define a multi-drug resistant organism (MDRO)
 Objectives. Outline. Define a multi-drug resistant organism (MDRO)") Multidrug Resistant Organisms (MDROs) Kasturi Shrestha, M.D. 05/11/2018 Objectives Define a multi-drug resistant organism (MDRO) Identify most challenging MDROs in healthcare Identify reasons for health
Multidrug Resistant Organisms (MDROs) Kasturi Shrestha, M.D. 05/11/2018 Objectives Define a multi-drug resistant organism (MDRO) Identify most challenging MDROs in healthcare Identify reasons for health
Antibiotics 201: Gramnegatives
 Antibiotics 201: Gramnegatives B. Joseph Guglielmo, Pharm.D. Professor and Dean School of Pharmacy University of California San Francisco Disclosures No potential conflicts of interest. 1 A 77 year old
Antibiotics 201: Gramnegatives B. Joseph Guglielmo, Pharm.D. Professor and Dean School of Pharmacy University of California San Francisco Disclosures No potential conflicts of interest. 1 A 77 year old
03/09/2014. Infection Prevention and Control A Foundation Course. Talk outline
 Infection Prevention and Control A Foundation Course 2014 What is healthcare-associated infection (HCAI), antimicrobial resistance (AMR) and multi-drug resistant organisms (MDROs)? Why we should be worried?
Infection Prevention and Control A Foundation Course 2014 What is healthcare-associated infection (HCAI), antimicrobial resistance (AMR) and multi-drug resistant organisms (MDROs)? Why we should be worried?
The role of carbapenems in the hospital
 The role of carbapenems in the hospital Matteo Bassetti, MD, PhD Infectious Diseases Division Santa Maria Misericordia University Hospital Udine, Italy Rationale for Antibiotic Optimizaton: Balancing The
The role of carbapenems in the hospital Matteo Bassetti, MD, PhD Infectious Diseases Division Santa Maria Misericordia University Hospital Udine, Italy Rationale for Antibiotic Optimizaton: Balancing The
1/30/ Division of Disease Control and Health Protection. Division of Disease Control and Health Protection
 Surveillance, Outbreaks, and Reportable Diseases, Oh My! Assisted Living Facility, Nursing Home and Surveyor Infection Prevention Training February 2015 A.C. Burke, MA, CIC Health Care-Associated Infection
Surveillance, Outbreaks, and Reportable Diseases, Oh My! Assisted Living Facility, Nursing Home and Surveyor Infection Prevention Training February 2015 A.C. Burke, MA, CIC Health Care-Associated Infection
Understanding the Hospital Antibiogram
 Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
Understanding the Hospital Antibiogram Sharon Erdman, PharmD Clinical Professor Purdue University College of Pharmacy Infectious Diseases Clinical Pharmacist Eskenazi Health 5 Understanding the Hospital
RESISTANT PATHOGENS. John E. Mazuski, MD, PhD Professor of Surgery
 RESISTANT PATHOGENS John E. Mazuski, MD, PhD Professor of Surgery Disclosures Contracted Research: AstraZeneca, Bayer, Merck. Advisory Boards/Consultant: Allergan (Actavis, Forest Laboratories), AstraZeneca,
RESISTANT PATHOGENS John E. Mazuski, MD, PhD Professor of Surgery Disclosures Contracted Research: AstraZeneca, Bayer, Merck. Advisory Boards/Consultant: Allergan (Actavis, Forest Laboratories), AstraZeneca,
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
VOLUME XXIX NUMBER 3 November 2014 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell SM MLS (ASCP), Marti Roe SM MLS (ASCP), Sarah Parker MD, Jason Child PharmD, and Samuel R.
Nosocomial Infections: What Are the Unmet Needs
 Nosocomial Infections: What Are the Unmet Needs Jean Chastre, MD Service de Réanimation Médicale Hôpital Pitié-Salpêtrière, AP-HP, Université Pierre et Marie Curie, Paris 6, France www.reamedpitie.com
Nosocomial Infections: What Are the Unmet Needs Jean Chastre, MD Service de Réanimation Médicale Hôpital Pitié-Salpêtrière, AP-HP, Université Pierre et Marie Curie, Paris 6, France www.reamedpitie.com
Introduction to Pharmacokinetics and Pharmacodynamics
 Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
Introduction to Pharmacokinetics and Pharmacodynamics Diane M. Cappelletty, Pharm.D. Assistant Professor of Pharmacy Practice Wayne State University August, 2001 Vocabulary Clearance Renal elimination:
LEARNING OBJECTIVES ANTIMICROBIAL USES AND ABUSES INFECTIOUS DISEASE SCARES
 LEARNING OBJECTIVES ANTIMICROBIAL USES AND ABUSES Goodbye to the Antibiotic Era? Glenn D. Bedsole, MD, FACP Infectious Disease Consultant 1. Be able to list 6 examples of resistant bacteria that present
LEARNING OBJECTIVES ANTIMICROBIAL USES AND ABUSES Goodbye to the Antibiotic Era? Glenn D. Bedsole, MD, FACP Infectious Disease Consultant 1. Be able to list 6 examples of resistant bacteria that present
ESISTONO LE HCAP? Francesco Blasi. Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano
 ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
ESISTONO LE HCAP? Francesco Blasi Sezione Medicina Respiratoria Dipartimento Toraco Polmonare e Cardiocircolatorio Università degli Studi di Milano Community-acquired pneumonia (CAP): Management issues
Pharmacodynamics as an Approach to Optimizing Therapy Against Problem Pathogens
 Pharmacodynamics as an Approach to Optimizing Therapy Against Problem Pathogens Jared L. Crandon, Pharm.D., BCPS Associate Director, Clinical and Experimental Pharmacology Center for Anti-Infective Research
Pharmacodynamics as an Approach to Optimizing Therapy Against Problem Pathogens Jared L. Crandon, Pharm.D., BCPS Associate Director, Clinical and Experimental Pharmacology Center for Anti-Infective Research
2009 ANTIBIOGRAM. University of Alberta Hospital and the Stollery Childrens Hospital
 2009 ANTIBIOGRAM University of Alberta Hospital and the Stollery Childrens Hospital Division of Medical Microbiology Department of Laboratory Medicine and Pathology 2 Table of Contents Page Introduction.....
2009 ANTIBIOGRAM University of Alberta Hospital and the Stollery Childrens Hospital Division of Medical Microbiology Department of Laboratory Medicine and Pathology 2 Table of Contents Page Introduction.....
Fundamental Concepts in the Use of Antibiotics. Case. Case. TM is a 24 year old male admitted to ICU after TBI and leg fracture from MVA ICU day 3
 Fundamental Concepts in the Use of Antibiotics Todd Miano, PharmD, MSCE Critical Care Pharmacist Pharmacoepidemiology Fellow Perelman School of Medicine at the University of Pennsylvania Case TM is a 24
Fundamental Concepts in the Use of Antibiotics Todd Miano, PharmD, MSCE Critical Care Pharmacist Pharmacoepidemiology Fellow Perelman School of Medicine at the University of Pennsylvania Case TM is a 24
Antimicrobial stewardship in managing septic patients
 Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
Antimicrobial stewardship in managing septic patients November 11, 2017 Samuel L. Aitken, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist, Infectious Diseases slaitken@mdanderson.org Conflict of interest
New Drugs for Bad Bugs- Statewide Antibiogram
 New Drugs for Bad Bugs- Statewide Antibiogram Felicia Matthews, Pharm.D., BCPS Senior Consultant, Pharmacy Specialty BE MedMined Services Disclosures Employee of BD Corporation MedMined Services Agenda
New Drugs for Bad Bugs- Statewide Antibiogram Felicia Matthews, Pharm.D., BCPS Senior Consultant, Pharmacy Specialty BE MedMined Services Disclosures Employee of BD Corporation MedMined Services Agenda
Rise of Resistance: From MRSA to CRE
 Rise of Resistance: From MRSA to CRE Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine SUPERBUGS (AKA MDROs) MRSA Methicillin-resistant S. aureus Evolution of Drug Resistance
Rise of Resistance: From MRSA to CRE Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine SUPERBUGS (AKA MDROs) MRSA Methicillin-resistant S. aureus Evolution of Drug Resistance
Intra-Abdominal Infections. Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018
 Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018") Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Intra-Abdominal Infections Jessica Thompson, PharmD, BCPS (AQ-ID) Infectious Diseases Pharmacy Clinical Specialist Renown Health April 19, 2018 Select guidelines Mazuski JE, et al. The Surgical Infection
Infectious Disease: Drug Resistance Pattern in New Mexico
 Infectious Disease: Drug Resistance Pattern in New Mexico Are these the world's sexiest accents? Obi C. Okoli, MD.,MPH. Clinic for Infectious Diseases Las Cruces, NM. Are these the world's sexiest accents?
Infectious Disease: Drug Resistance Pattern in New Mexico Are these the world's sexiest accents? Obi C. Okoli, MD.,MPH. Clinic for Infectious Diseases Las Cruces, NM. Are these the world's sexiest accents?
New Antibiotics for MRSA
 New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
New Antibiotics for MRSA Faculty Warren S. Joseph, DPM, FIDSA Consultant, Lower Extremity Infectious Diseases Roxborough Memorial Hospital Philadelphia, Pennsylvania Faculty Disclosure Dr. Joseph: Speaker
RCH antibiotic susceptibility data
 RCH antibiotic susceptibility data The following represent RCH antibiotic susceptibility data from 2008. This data is used to inform antibiotic guidelines used at RCH. The data includes all microbiological
RCH antibiotic susceptibility data The following represent RCH antibiotic susceptibility data from 2008. This data is used to inform antibiotic guidelines used at RCH. The data includes all microbiological
10 Golden rules of Antibiotic Stewardship in ICU. Jeroen Schouten, MD PhD intensivist, Nijmegen (Neth) Istanbul, Oct 6th 2017
 Istanbul, Oct 6th 2017") 10 Golden rules of Antibiotic Stewardship in ICU Jeroen Schouten, MD PhD intensivist, Nijmegen (Neth) Istanbul, Oct 6th 2017 10 golden rules of Antibiotic Stewardship in the ICU ID, Pharma & Micro advice
10 Golden rules of Antibiotic Stewardship in ICU Jeroen Schouten, MD PhD intensivist, Nijmegen (Neth) Istanbul, Oct 6th 2017 10 golden rules of Antibiotic Stewardship in the ICU ID, Pharma & Micro advice
Infectious Disease Issues in the Intensive Care Unit
 Infectious Disease Issues in the Intensive Care Unit Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Overview Emerging antibiotic
Infectious Disease Issues in the Intensive Care Unit Catherine Liu, M.D. Assistant Clinical Professor Division of Infectious Diseases University of California, San Francisco Overview Emerging antibiotic
Childrens Hospital Antibiogram for 2012 (Based on data from 2011)
") Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
Childrens Hospital Antibiogram for 2012 (Based on data from 2011) Prepared by: Department of Clinical Microbiology, Health Sciences Centre For further information contact: Andrew Walkty, MD, FRCPC Medical
CONTAGIOUS COMMENTS Department of Epidemiology
 VOLUME XXIII NUMBER 1 July 2008 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell, SM (ASCP), Marti Roe SM (ASCP), Ann-Christine Nyquist MD, MSPH Are the bugs winning? The 2007
VOLUME XXIII NUMBER 1 July 2008 CONTAGIOUS COMMENTS Department of Epidemiology Bugs and Drugs Elaine Dowell, SM (ASCP), Marti Roe SM (ASCP), Ann-Christine Nyquist MD, MSPH Are the bugs winning? The 2007
Antibiotic Resistance. Antibiotic Resistance: A Growing Concern. Antibiotic resistance is not new 3/21/2011
 Antibiotic Resistance Antibiotic Resistance: A Growing Concern Judy Ptak RN MSN Infection Prevention Practitioner Dartmouth-Hitchcock Medical Center Lebanon, NH Occurs when a microorganism fails to respond
Antibiotic Resistance Antibiotic Resistance: A Growing Concern Judy Ptak RN MSN Infection Prevention Practitioner Dartmouth-Hitchcock Medical Center Lebanon, NH Occurs when a microorganism fails to respond
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities.
 Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
Table 1. Commonly encountered or important organisms and their usual antimicrobial susceptibilities. Gram-positive cocci: Staphylococcus aureus: *Resistance to penicillin is almost universal. Resistance
EARS Net Report, Quarter
 EARS Net Report, Quarter 4 213 March 214 Key Points for 213* Escherichia coli: The proportion of patients with invasive infections caused by E. coli producing extended spectrum β lactamases (ESBLs) increased
EARS Net Report, Quarter 4 213 March 214 Key Points for 213* Escherichia coli: The proportion of patients with invasive infections caused by E. coli producing extended spectrum β lactamases (ESBLs) increased
3/20/2011. Code 215 of Hammurabi: If a physician performed a major operation on
 The Good Antibiotics: the Good, the Bad and the Ugly John P. Cello, MD Professor of Medicine and Surgery, University of California, San Francisco Most organisms can be readily identified by culture, special
The Good Antibiotics: the Good, the Bad and the Ugly John P. Cello, MD Professor of Medicine and Surgery, University of California, San Francisco Most organisms can be readily identified by culture, special
Antibiotic Updates: Part I
 Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Antibiotic Updates: Part I Fredrick M. Abrahamian, DO, FACEP, FIDSA Health Sciences Clinical Professor of Emergency Medicine David Geffen School of Medicine at UCLA Los Angeles, California Financial Disclosures
Standing Orders for the Treatment of Outpatient Peritonitis
 Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
Standing Orders for the Treatment of Outpatient Peritonitis 1. Definition of Peritonitis: a. Cloudy effluent. b. WBC > 100 cells/mm3 with >50% polymorphonuclear (PMN) cells with minimum 2 hour dwell. c.
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams
 DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
DETERMINANTS OF TARGET NON- ATTAINMENT IN CRITICALLY ILL PATIENTS RECEIVING β-lactams Jan J. De Waele MD PhD Surgical ICU Ghent University Hospital Ghent, Belgium Disclosures Financial: consultancy for
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship
 Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Methicillin-Resistant Staphylococcus aureus Nasal Swabs as a Tool in Antimicrobial Stewardship Natalie R. Tucker, PharmD Antimicrobial Stewardship Pharmacist Tyson E. Dietrich, PharmD PGY2 Infectious Diseases
Antimicrobial Stewardship Strategy: Antibiograms
 Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Antimicrobial Stewardship Strategy: Antibiograms A summary of the cumulative susceptibility of bacterial isolates to formulary antibiotics in a given institution or region. Its main functions are to guide
Hospital-acquired pneumonia (HAP) is the second
 is the second") Guidelines and Critical Pathways for Severe Hospital-Acquired Pneumonia* Stanley Fiel, MD, FCCP Hospital-acquired pneumonia (HAP) is associated with high morbidity and mortality. Early, appropriate, and
Guidelines and Critical Pathways for Severe Hospital-Acquired Pneumonia* Stanley Fiel, MD, FCCP Hospital-acquired pneumonia (HAP) is associated with high morbidity and mortality. Early, appropriate, and
ESBL Producers An Increasing Problem: An Overview Of An Underrated Threat
 ESBL Producers An Increasing Problem: An Overview Of An Underrated Threat Hicham Ezzat Professor of Microbiology and Immunology Cairo University Introduction 1 Since the 1980s there have been dramatic
ESBL Producers An Increasing Problem: An Overview Of An Underrated Threat Hicham Ezzat Professor of Microbiology and Immunology Cairo University Introduction 1 Since the 1980s there have been dramatic